Your Guide to Selecting the Right Laser Safety Standard
As more and more workplaces in the United States begin to implement laser technology, the need to stay on the leading edge of laser safety updates becomes more important. Laser Safety Officers (LSOs) know that the best way to stay informed about laser safety standards and practices is to become familiar with the American National Standards Institute’s (ANSI) Z136 series of laser safety standards.
Job shops, researchers and medical professionals want to prevent accidents. By following the ANSI standards, you are promoting a safe work environment while avoiding costly accidents and improving your overall safety footprint.
Having the laser safety standard most applicable to your profession is essential to maintaining a successful laser safety program. They are the only laser safety guidelines that are nationally accepted by a variety of organizations, including the Occupational Safety and Health Administration (OSHA) and The Joint Commission (TJC). And since the Laser Institute of America (LIA) serves as the publisher of the series, you can be confident that you are purchasing the most current laser safety information available.
The Z136 standards are revised after an extensive review process is completed to ensure that all information is correct and up-to-date. This process is led by one main committee, and further composed of an oversight committee, an editorial working group, five technical committees and 10 “standards” committees that are each responsible for a specific standard. Once a subcommittee has completed a standard, the other committees review the document — a process that can take several years.
Before publishing, the American National Standards Institute approves the document. However, ANSI does not approve the content. It approves the process by which the document was revised to “verify that the principles of openness and due process have been followed and that a consensus of all interested stakeholder groups has been reached.” Once ANSI has approved the document, the secretariat makes any necessary formatting and grammatical edits before being sent to print.
The most recent update to the laser safety standards is the ANSI Z136.6 Safe Use of Lasers Outdoors. The 2015 revision expands upon the previous version and hopes to meet the evolving needs of outdoor laser operators. Designed for use by laser-light show operators, scientific and astronomical research, the Department of Energy, and the Department of Defense, the revised ANSI Z136.6 provides guidance for the safe use of lasers and laser systems (180 nm to 1 mm) that could possibly be hazardous in outdoor environments where open-beam paths are necessary.
There are a number of additional Z136 laser safety standards available that cater to a variety of industries and professionals, not just those that use laser technology outdoors, including:
ANSI Z136.1 Safe Use of Lasers
ANSI Z136.2 Safe Use of Optical Fiber Communication Systems Utilizing Laser Diode and LED Sources
ANSI Z136.3 Safe Use of Lasers in Health Care
ANSI Z136.4 Recommended Practice for Laser Safety Measurements for Hazard Evaluation
ANSI Z136.5 Safe Use of Lasers in Educational Institutions
ANSI Z136.7 Testing and Labeling of Laser Protective Equipment
ANSI Z136.8 Safe Use of Lasers in Research, Development, or Testing
ANSI Z136.9 Safe Use of Lasers in Manufacturing Environments
As the parent document of the ANSI Z136 standards, Z136.1 is the number one seller and the standard that most laser safety officers purchase, according to Barbara Sams, the Executive Director of the Board of Laser Safety. This tool is essential for any LSO to have on hand.
In addition to this tool, having the laser safety standard that’s most applicable to your industry is another great way to keep your laser safety program current, as it can serve as both a reference tool and a guide for your laser safety initiatives. Because laser safety measures are different for each industry, control measures for one industry can be very different from another. In health care, you would use Z136.3; in manufacturing, you would use Z136.9; and so on. Control measures for one area of practice do not necessarily apply to the other.
If you are just now beginning your journey as a Laser Safety Officer, the Z136 standards are a great tool to have while you complete the necessary training and develop your laser safety program. Thesestandards provide protocols and procedures you can use to create a laser safety program in a facility that may not have had one before. By following the guidelines outlined in the standards, you are protecting your employees and satisfying OSHA requirements that state all employers must provide a safe workplace that meets a national consensus standard, in this case laser safety.
The photonics industry is ever-changing, and LIA is dedicated to helping LIA members and non-members alike get the resources they need to ensure their laser safety programs are safe and up-to-date. If you have purchased one of the Z136 standards in the past, LIA will send you an email notification when the standard is revised — allowing you to stay on the forefront of new laser safety information.
You may purchase any of the Z136 laser safety standards in print or digital format on LIA’s website. If you have any questions about the ANSI standards or LIA laser safety training options, you may contact us online.
In the words of Sidney Dekker, an expert in learning from adverse events, “the key to an investigation is not to point out where people went wrong, but to understand how their assessments and actions made sense inside that situation at the time.”1
As the laser safety officer, key elements to the investigation phase include:
Visit the location where the event took place
Interview those who were there at the time of the accident
Take pictures; capture the scene
Get a clear explanation of the work being done (consider process mapping)
The new view of safety challenges findings reported in the literature, such as 67 percent of medical laser accidents are attributed to operator error and demands that we look deeper into why these errors were made2. In the words of Trevor Kletz, “listing human error as the cause of an accident is about as helpful as listing gravity as the cause of a fall. It may be true, but it does not lead to constructive action. 3
To truly learn what contributed to the event, the laser safety officer must ensure ‘psychological safety’ of the individuals being interviewed. It is essential that the message be clear that this is a non-punitive process, with the focus of learning and improving, and that messaging is consistent from the manager level to senior leadership.
As in nearly any adverse event, one can point to a procedure or policy that was violated; it is often the first reaction of leadership to suggest that the individual who violated that procedure be held accountable. In deciding whether or not this is appropriate, an important test, known as the ‘substitution test’ is conducted. This involves asking the question whether another individual with the same information under the same circumstances might have made the same decision. If the answer is yes, then it is not appropriate to look at individual performance, but rather to look at the system in which the event took place.
Investigation & Analysis of Incidents The following example is roughly based on Incident no.7, reported to the British Medical Laser Association, and discussed in the paper by Moseley2:
Scenario 1: “Description: Laser used in conjunction with a bronchoscope, LPA was called because a registrar had corneal damage. The procedure had taken about 1 h. Registrar claimed she had worn the glasses. The glasses and equipment were tested and found to be in good order. Follow up and outcome: The scarring resolved and the problem was never solved. No legal action followed. The totally unfounded suspicion of the LPA is that the glasses were abandoned and optimism relied upon instead.”
Concluding that an injury occurred because laser protective eyewear was not worn may be true, but does not lead to constructive action. If one explores why the laser protective eyewear was not warn, a host of reasons could surface;
laser protective eyewear does not fit comfortably
laser protective eyewear color distortion interferes with view of biological tissues
laser operator wears prescription glasses, eyewear does not fit over his/her glasses
laser eyewear for multiple lasers is stored in one drawer, making it is possible to select the incorrect eyewear
the manufacturer (‘expert’) from the company never wears laser protective eyewear when he visits the site
Each of these reasons leads to a different corrective action.
Why-Why Method One method used in patient safety is the “Why-Why method,” where you repetitively ask “why” to arrive at the deeper rooted factors that led to the event. In this example, we might ask:
Q: Why was LPE not worn?
A: “It was not available.”
Q: Why was it not available?”
A: “We don’t know what to order.”
Q: “Why don’t you know what to order?”
A: “The nurse that was our laser safety expert left our team, and no one has replaced her.”
We see by drilling deeper, buying an additional pair of laser protective eyewear would not have resolved the main underlying issue of not having a laser safety specialist supporting the surgical group.
Constellation Mapping A method of analyzing adverse events, known as a ‘constellation mapping’ guides the analysis team to consider how various factors contributed to the outcome:
patient
health care provider (laser operator)
team
organization
environment
equipment
task
This method, introduced in the Canadian Incident Analysis Framework, is a powerful tool in shifting from blaming individuals (“operator error”), to identifying systems fixes that will prevent future adverse events.4 This type of ‘systems’ accident model replaces earlier models that sought out a single ‘root cause.’ The findings can then be organized in to a matrix format i.e., constellation map, as shown in Figure 1.
Figure 1. Constellation map framework [4]
This constellation map is populated with the information gathered during the interview phase. The laser safety officer typically conducts interviews with frontline staff themselves. In interviewing, keeping the questions broad, such as, “tell me what you remember about the event,” often yields the most information. Additional questions can be asked to clarify points, or assess the laser safety culture within the team. If the questions are too scripted, and asked one after the other without giving the individual the chance to first share their story, it can feel like an inquisition rather than non-punitive learning opportunity. It is important to ask the interviewee their ideas for improvements. Often the best suggestions come from the frontlines
It is important to conduct this exercise as a team, to include key perspectives such as a nurse and physician perspective in the health care setting.
The following example is roughly based on Incident no.7, reported to the British Medical Laser Association, and discussed in the paper by Moseley2:
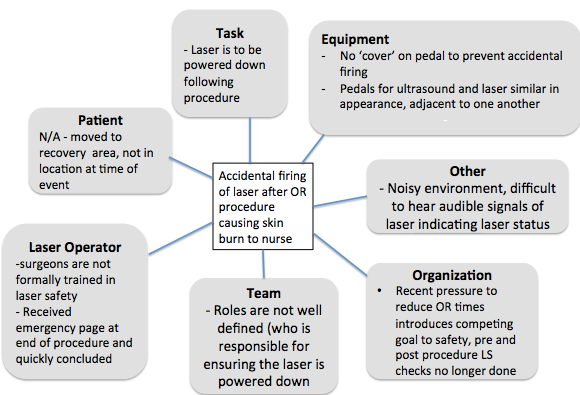
Scenario 2: A laser was fired after a surgical procedure was concluded, when an OR staff cleaning up the OR stepped on the laser pedal, resulting in a skin burn to a fellow nurse who was also in the area.
Rather than quickly concluding that this was operator error (forgetting to put the laser in standby after the procedure), interviews with the surgical team will allow the review team to build a deeper understanding of contributing factors. It is essential in interviews to emphasize that this is a non-punitive process with an emphasis on learning. The shifting of focus to the individual operator to the system, is known as “Systematic Safety Analysis.” A thorough guide for this approach is available online from the Health Quality Council of Alberta.5
In the example of the ‘accidental firing,’ one might find the following through interviews:
The laser pedal does not have a safeguard that would prevent accidentally stepping on ‘fire’ button.
The pedals for the laser and ultrasound are side by side, misfiring of the laser is not uncommon, this is just the first time it lead to injury.
There is no formal laser safety training for surgeons who operate lasers – surgeons visit a site to learn how to use the laser from an experienced surgeon, followed by a period of support from company rep.
Onsite training records show only nurses have attended laser safety training sessions.
The audible indicators that the laser is in the ‘ready’ state are difficult to hear in the noisy or setting.
Organizational pressure to reduce OR time, pre and post procedure LS checklist no longer done.
The surgeon had received an emergency page as the procedure was ending.
Nurse A thought the surgeon had powered down the laser before leaving. The surgeon is used to working with Nurse B who always takes care of powering down the laser at the end of the procedure.
The populated constellation map for Scenario 2 is shown in Figure 2.
Figure 2. Populated constellation map for ‘accidental firing of laser’ scenario
We now have a much richer understanding of the factors that contributed to this event, and many more recommendations to consider than we would if we had concluded ‘operator error’ was responsible.
Recommendations in Response to Incident Continuing with reference to Scenario 2, if we had concluded ‘operator error’ was responsible, we likely would have had one follow up action taking the form of a memo or email to all operators of surgical lasers to ensure the laser is put in standby mode or powered off when not in use.
A method used widely in the patient safety community is the hierarchy of effectiveness of corrective actions as shown in Figure 3.5 Referring to the ‘hierarchy of effectiveness’ of corrective actions, shown in Figure 3, this would be considered ‘inform/educate,’ considered the weakest intervention.
This also reinforces to the entire team that the organization follows up to adverse events with a ‘shame and blame’ approach. It is likely that when the email is sent, everyone knows who exactly forgot to turn off the laser that day.
Figure 3. Hierarchy of effectiveness of corrective actions, established by the Institute of Safer Medication Practices [5]
Through taking a systems approach, and carrying out the exercise of constellation mapping, we have arrived at many more contributing factors that can be addressed through recommendations. In formulating recommendations, it is important to consider this relative hierarchy. Recommendations to consider based on these findings might include:
Equipment: Ensure laser pedals are covered. Consider means of distinguishing ultrasound pedal from laser pedal (geographical separation, visual distinction) to reduce risk of accidental firing.
Standardize the roles in the OR team, including who is responsible for pre- and post- laser check.
Training: Outreach aimed at physician group (rounds, explore whether CME points can be awarded for laser safety training).
For Medical Laser Safety Officers that find it challenging to engage physicians in the laser safety program at their facility, the Institute for Healthcare Improvement white paper “Engaging Physicians in a Shared Quality Agenda” provides strong guidance.6
Sharing Lessons Learned To close the loop, and strengthen the laser safety culture, it is essential to share lessons learned from laser safety incidents. Some methods of sharing include:
Provide a complete report to administration and the LS Committee and regulating body.
Write a Lessons Learned report to share with other laser users (not to blame but rather to point out contributing factors and corrective actions).
Incorporate case studies in laser safety training.
Present the adverse event and lessons learned at a conference.
When other laser users see the ‘systems approach’ taken in response to adverse events, they will be more likely to come forward and report adverse events.
It is important to stress that this methodology can be applied to ‘near misses’ or ‘close calls’ with equally as rich learning. This is, of course, the preferred method of learning, when harm has not occurred. A non-punitive response to adverse events will have a positive effect on the reporting culture, including the reporting of ‘near misses’ or ‘close calls.’
Conclusions It is a worthwhile exercise for Medical Laser Safety Officers to become skilled at applying current methodology used in patient safety to learn from adverse events. Taking a systems approach, and identifying the many contributing factors detailed in Figure 2, leads to constructive change and improvement to the laser safety program.
References
[1] Dekker, Sidney (2006), The Field Guide to Understanding Human Error.
[2] Moseley, Harry, (2004) Operator error is the key factor contributing to medical laser accidents” Lasers in Medical Science 19; 105-111.
[3] Kletz, Trevor A. (1993) Lessons from disaster, How Organizations Have No Memory and Accidents Recur. Gulf Professional. ISBN 978-0884151548, p510.
[4] Canadian Patient Safety Institute (CPSI). (2012) Canadian incident analysis framework, p 44.
[5] Duchscherer C., Davies, J.M. (2012) Systematic Systems Analysis: A Practical Approach to Patient Safety Reviews” Health Quality Council of Alberta (HQCA). Available online at www.hcqa.ca
[6] Reinertsen JL, Gosfield AG, Rupp W, Whittington JW. (2007) Engaging Physicians in a Shared Quality Agenda. IHI Innovation Series white paper. Cambridge, MA: Institute for Healthcare Improvement; (Available on www.IHI.org)
Jodi Ploquin is a Certified Laser Safety Officer (CMLSO) specializing in medical, academic and commercial applications in laser safety with KRMC Inc. Liz Krivonosov is President of KRMC, a firm specializing in the risk management of hazardous materials. She is a Professional Engineer and a Certified Industrial Hygienist.
Orlando, FL (Jan. 20, 2016) – With the ever-increasing number of laser end-users, companies are continuously looking to implement cost-effective and efficient laser safety programs for new and current employees. In an effort to offer Laser Safety Officers (LSOs) the best training tools available, Laser Institute of America (LIA) has updated its 2009 Mastering Light: An Introduction to Laser Safety & Hazards training video. LIA aims to provide the best methods for successful laser safety training in the constantly changing, fast-paced field of laser technology and has done so once again with the 2016 edition of Mastering Light:An Introduction to Laser Safety & Hazards — now available for pre-order.
For years, the Mastering Light: An Introduction to Laser Safety & Hazards DVD has provided LSOs with a training tool that is not only easy to administer, but also effective in properly training employees, researchers and students alike. Like its predecessor, the new version will still outline the important safety rules and regulations employees must know in the field. However, the latest edition of the video will now feature new footage and updated information to provide employees with the best safety training possible. In addition, LIA is continuing its tradition of striving to improve the training process – both for trainees and the LSOs tasked with the critical job of educating employees – by offering both a DVD and a digital version with the purchase of the video. The digital version will be available for viewing at lia.org, where it will appear under users’ downloads.
Written and produced by LIA, Mastering Light: An Introduction to Laser Safety & Hazards fulfills both the ANSI Z136.1 Safe Use of Lasers and the Occupational Safety and Health Administration’s (OSHA) laser safety requirements for employees who routinely work with or who potentially could be exposed to Class 3B or Class 4 laser radiation.
This video informs viewers on a multitude of important concepts to ensure their safety in the field. It reviews the physics of a laser, the classification of lasers by hazard potential — Class 1M, Class 2, Class 2M, Class 3R, Class 3B, and Class 4 — and the definition and duties of a Laser Safety Officer. It discusses the two categories of laser hazards: beam and non-beam. It includes a clear explanation of labels and signs, specifically the new sign design and the grandfathering of the old sign designs in previous versions of the ANSI Z136.1. Viewers also receive information about control measures — from administrative and engineering to personal protective equipment, as well as fiber laser applications. In addition, the video features revised information and footage of Class 1M and 2M military lasers.
“LIA included more information on fiber and diode lasers,” Jeannette Gabay, CAE, stated. “We also included clearer descriptions of the differences between signs and labels, as well as differences between regulatory agencies, such as FDA/CDRH and OSHA.”
These revisions will provide LSOs with an even more thorough training tool to ensure employees’ safety in the field. And, to further aid in the training process, LIA has created an additional facet to the Mastering Light: An Introduction to Laser Safety & Hazards program: A quiz. This quiz — included in the DVD packaging — gives LSOs the ability to effectively determine employees’ understanding of the video’s concepts and safety information. By implementing this new addition, LIA hopes to further increase the effectiveness of its training tool.
The new Mastering Light: An Introduction to Laser Safety & Hazards video will be available for purchase in early 2016. LIA members can purchase the single user product for $450 or the site license version for $850, while non-members can purchase the single user product for $495 or the site license version for $895.
To learn more about LIA’s well-known training tool, Mastering Light: An Introduction to Laser Safety & Hazards, and to purchase a copy for your company, visit: www.lia.org/store.
About LIA
The Laser Institute of America (LIA) is the professional society for laser applications and safety serving the industrial, educational, medical, research and government communities throughout the world since 1968. www.lia.org, 13501 Ingenuity Drive, Ste 128, Orlando, FL 32826, +1.407.380.1553.
Orlando, FL (Jan. 5, 2016) – After ten years, the long awaited revision of the ANSI Z136.6 Safe Use of Lasers Outdoors is here! This standard, now available for purchase, sees updates to nearly the entire document – expanding and modernizing the established topics and sections.
The 2015 revision of the ANSI Z136.6 Safe Use of Lasers Outdoors is the premier safety standard and a necessary tool for anyone operating a laser system in an open-air environment. This newly revised document provides guidance for the safe use of potentially hazardous lasers and laser systems (180 nm to 1 mm), where the establishment of open beam paths is necessitated. When used in conjunction with the ANSI Z136.1 Safe Use of Lasers, the Z136.6 ensures that your outdoor laser applications are in conformity with the latest safety guidelines.
This latest edition was created with the goal to update, clarify, and streamline an already established, recognized standard to better reflect today’s outdoor laser operator’s needs.
Some of the changes to the 2015 edition include:
Single column format and index for improved readability and searchability, and color added to figures for ease of use.
Added definition of “Control Measures” with explanation of preferred categories.
Complete rewrite of the Control Measures section to include the removal of most manufacturer-specific requirements, and the addition of an expanded and standalone military-specific section.
Metric unit standardization across the standard means no more pesky conversions.
New definitions and expanded content for visual interference zones around airports and general critical tasks.
FAA coordination requirements clarified.
Laser hazard classification revised to include a comparison table between 2000 & 2014 version of ANSI Z136.1 and better explain the purpose and types of hazard classification.
General section and formatting updates to better reflect today’s jargon.
Order your copy today and be one of the first to own this long awaited revision of the ANSI Z136.6 standard. For more information, visit www.lia.org/store to see this and all the other ANSI Z136 laser safety standards.
About LIA
The Laser Institute of America (LIA) is the professional society for laser applications and safety serving the industrial, educational, medical, research and government communities throughout the world since 1968. www.lia.org, 13501 Ingenuity Drive, Ste 128, Orlando, FL 32826, +1.407.380.1553.
If there’s one image that stays with you after the International Laser Safety Conference, it’s an image of the blowtorch effect caused by a laser striking an oxygen-filled endotracheal tube.
Screen grab from a YouTube video showing an endotracheal tube being set afire by a CO2 laser. (Click image to watch video).
Another powerful visual is imagining a concerned — and empowered — laser safety officer walking away from a potentially dangerous operating room situation if a laser surgery seems about to go awry.
Yet another indelible image is picturing a 53-year-old grandmother undergoing a routine 10-minute laser procedure to remove vocal cord polyps — only to have her airway seared after a series of apparent educational and procedural lapses.
Some might say pointing out such dire occurrences is merely an attempt to frighten or be provocative. But there’s really no way to make an inherently horrific occurrence like an airway fire any scarier than it is.
Perhaps more worrisome is the fact that so many more medical LSOs should be certified to take the reins of laser safety in health-care facilities large and small. The need is evident as lasers grow in importance as a surgical and therapeutic tool.
Further evidence of the need for certified medical laser safety officers was provided by attorney Matthew Wojcik of Seattle firm Bullivant Houser Bailey, who detailed the 2012 case of the aforementioned 53-year-old Washington state woman who eventually died from injuries sustained from an airway fire that started about eight-and-a-half minutes into her surgery. According to Wojcik, who represented the laser manufacturer, the surgeon, anesthesiologist and “laser safety nurse” all testified to varying degrees of understanding or even awareness of hospital laser safety protocols, their application and the laser safety committee’s role.
With no CMLSO in place, potential red flags during the procedure — including the laser being set to 18 watts and the oxygen not being turned down from 100 percent to around 30 percent — went unheeded. In fact, the hospital’s previous LSO had left about two years before the incident.
Ultimately, the hospital reached a $12 million settlement with the patient before trial; the patient was awarded $18 million after a trial. (The laser manufacturer was dismissed from the lawsuit prior to trial; the maker of the endotracheal tube was spared from blame in the trial.)
And to think that it might only have cost about $3,500 to properly train and certify a CMLSO who could have been empowered enough to notice anomalies in the procedure and address them — or even postpone the surgery.
It seems hard to argue that the added insurance of naming, training and certifying a CMLSO is worth the cost, given the potentially severe toll a laser surgery gone wrong might take.
A quick look at the list of dozens of CMLSOs certified by the Board of Laser Safety shows that many facilities across the U.S. are committed to investing in the soundness of laser policies and procedures. And yet, a recent survey by UHS Surgical Services indicated that about 40 percent of the 266 health-care facilities responding did not have an LSO or safety program in place.
Where do you stand? Is certifying a medical LSO essential or a luxury?
Geoff is LIA’s communications director. Contact him at ggiordano@lia.org to share your experiences with lasers, sound off on issues regarding any facet of laser technology, suggest stories or offer your commentary with a guest article or blog post.




![Figure 1. Constellation map framework [4]](https://www.laserstoday.com/wp-content/uploads/2016/06/Figure-1.png)


![Figure 3. Hierarchy of effectiveness of corrective actions, established by the Institute of Safer Medication Practices [5]](https://www.laserstoday.com/wp-content/uploads/2016/06/Figure-3-e1465960164334.png)



